|
| |
Issue no. 7 - November 1981
pdf
 version of this Issue version of this Issue
|
There is much information in this issue that is valuable
and useful. Online readers are reminded, however, that treatment guidelines and health
care practices change over time. If you are in doubt, please refer to
WHO's up-to-date Dehydration Treatment
Plans.
|
Pages 1-8 Diarrhoea Dialogue Online Issue 7 -
November 1981
|
DDOnline
Diarrhoea Dialogue Online Issue 7 November 1981
 Page 1 2
Page 1 2
Cause - And Effect
Acute diarrhoea can cause life-threatening dehydration very quickly. Rehydration must
start at once and primary health care workers need to make decisions about treatment based
on signs, symptoms and their own experience. Long before the actual cause of the diarrhoea
can be identified, the patient may either be getting better - or be dead.
|
Making the best guess possible on the basis of signs,
symptoms and past experience. A voluntary health auxiliary brings primary health care
to a family near Lake Titicaca in Peru.
WHO photograph by D. Henrioud
|
 |
Many health workers do not have access to laboratory facilities to discover which
infectious organisms in the gut are causing diarrhoea. They can, nevertheless, still save
lives because rehydration therapy - particularly oral rehydration therapy - is the key
factor in the management of acute diarrhoea, whatever the cause. However, identifying the cause is important when decisions need to be made about
treating people with drugs - or about control measures in the family or community, such as
improved food handling, encouragement of breastfeeding, cleaner water supplies and better
sanitation. This issue of Diarrhoea Dialogue looks at the various causes of
diarrhoeal disease because, eventually, improved knowledge of this area will bring more
effective cure and more appropriate prevention. The information in this issue should also
assist primary health care workers in remote areas to make the best guess possible about
causes so that standard treatments can be modified to give quicker results. K.M.E. and W.A.M.C.
|
In this issue...
- David Candy looks at the causes of childhood diarrhoea
- Cholera up-date
- Clinician's guide to aetiology
|
|
DDOnline
Diarrhoea Dialogue Online Issue 7 November 1981
1 Page 2 3
Publications
Paediatricians in developing countries often have limited access to libraries and have
difficulty in keeping up-to-date with current developments in their field. Two recent
publications should help to fill this gap. Both are expensive but, if affordable, merit
their cost as they provide excellent 'state-of-the-art' reviews and reference sources.
- Secretory Diarrhoea (Edited by Michael Field) 1980 237pp. Price $30.00. Available
from: Williams & Wilkins Company, 68 Upper Richmond Road, Putney, London SW15 2SF, UK.
- Paediatrics in the Tropics (Edited by R. G. Hendrickse) 1981 392pp. Price
£20.00. Available from: Oxford University Press, Oxford OX2 6DP, UK.
Also available, free of charge, is a report recently published by the Committee on
International Nutrition Programs - Management of the Diarrhoeal Diseases at Community
Level (Edited by Richard Cash). The report focuses on oral rehydration and continued
feeding in the management of acute diarrhoeal diseases. To obtain a copy, write to:
National Academy Press, 2101 Constitution Avenue, Washington DC 20418, USA. Diarrhoea agents in the environment
All the diarrhoeas discussed in this issue that are caused by intestinal pathogens are
transmitted from the anus of the infected person to the mouth of a susceptible person.
This faecal-oral transmission can take place directly (on hands for instance) or via
contaminated food or water. To control diarrhoea transmission it is necessary to have
information on the occurrence and survival of the various pathogens in the environment and
to understand the effects of water and sewage treatment processes upon them. We know a great deal about the environmental properties of the "classical"
diarrhoea agents. This is especially true for Salmonellae and, to a lesser extent, for
Shigellae, vibrios and Entamoeba histolytica. We also know much about the behaviour
of commensal E. coli in the environment, although we do not yet know whether the
toxigenic and invasive strains of E. coli are similar to the non-pathogenic strains
in their environmental properties.
|
Rotavirus
in a faecal sample from a child with diarrhoea.
Electronmicrograph provided by I. L. Chrystie We know very little about the environmental properties of the more recently recognized
diarrhoea agents. Work on rotavirus, and other viruses. is only just beginning and there
are still enormous technical problems in isolating these organisms from the environment
because they do not grow well in cell cultures. Environmental information about Campylobacter,
ETEC and Yersinia is now being collected. The laboratory difficulties have
been, or soon will be, overcome and we can expect an explosion of literature on these and
other pathogenic enteric bacteria in the next few years. The same is true for the parasite
Giardia lamblia.
|
 |
Recent reviews of enteroviruses (which, in the absence of laboratory techniques
provide the best approximation of rotavirus) and Vibrio cholerae in the environment
have been published in Tropical Diseases Bulletin, Vol 78, pp 185-230 and pp
865-880. Bottles on prescription
|
Breastfeeding in Papua New Guinea.
Photograph by Dr Michael Gracey In Diarrhoea Dialogue 3, we mentioned that since
1977, feeding bottles have only been available on prescription in Papua New Guinea. Recent
information from Port Moresby General Hospital indicates that this policy is having a
significant impact. The number of shops selling feeding bottles has greatly reduced;
breastfeeding has increased; and general awareness of the dangers of bottle-feeding
without adequate safeguards has grown.
|
 |
All these factors have played an important role in reducing the number of
gastroenteritis admissions to the hospital and associated deaths in infants less than six
months of age.(1) (1) Impact of Sales Control of Feeding Bottles 1981 Weekly Epidemiological Record
No. 16 April 24: 126.
|
|
DDOnline
Diarrhoea Dialogue Online Issue 7 November 1981
2 Page 3 4
The most feared of the diarrhoeal diseases
"Cholera remains an enigmatic disease and has by no means yielded up all its
secrets. There is much to be done in both the epidemiology and the immunology of cholera;
many questions remain unanswered"(1) Historically, cholera has always been the most feared of the diarrhoeal diseases
because it can spread fast and kill its victims within a matter of hours if treatment is
not readily available. It therefore continues to be one of the four diseases subject to
the International Health Regulations (2), under which member states are required to notify
the presence of cases to WHO. Although the Regulations have not prevented the
international spread of cholera, they have helped to keep WHO and public health
authorities informed of the global epidemiological situation and alert to any possible
risk. Seventh pandemic The seventh pandemic of cholera, which began in Indonesia in 1961 and is caused by the
El Tor biotype of Vibrio cholerae, has now spread to more than 90 countries in
Africa, Asia, Europe, North America and Oceania. Although there have been periods of
respite, the pandemic still shows no signs of decreasing (Table 1). In many countries
cholera has become endemic, creating a greater risk of spread to new areas. However,
experience in developed countries has repeatedly shown that, when importations of cholera
are detected promptly, subsequent spread within a country can be prevented.
|
TABLE 1.
Global cholera situation, 1975-1980 |
| |
1975 |
1976 |
1977 |
1978 |
1979 |
1980 |
| Number of countries reporting cholera |
29 |
27 |
35 |
40 |
43 |
32 |
| Number of new countries infected |
1 |
- |
3 |
8 |
2 |
- |
| Number of cases reported |
92,123 |
66,020 |
58,087 |
74,632 |
56,813 |
36,815 |
In 1980, as in previous years, the great majority of reported cases
occurred in Africa (17,675 cases in 14 countries) and Asia (19,108 cases in 15 countries)
( 3). In addition, a total of 32 cases occurred in nine countries in America, Europe and
Oceania, but 27 of these were imported and only five were indigenous cases. While no new
countries were infected that year, and the total number of countries reporting the disease
declined substantially, there were a number of countries where cholera reappeared,
sometimes after an absence of several years. This is, however, a common pattern. Resurgence in the Eastern Mediterranean This year, a total of 20,346 cases have been reported up to late September and
notifications are still far from complete. Twelve countries in Africa and 15 in Asia have
notified the presence of cholera, and small numbers of cases have again been reported by
the USA and Australia. No new countries have been infected. Of interest is the apparent
resurgence of cholera in the Eastern Mediterranean area, where an outbreak of 869 cases
occurred in Jordan in July/August. Small numbers of cases were also reported in the Gaza
Strip and the West Bank, and in Iran there have been 3,030 cases reported altogether since
mid-April. Cholera control
|
Preventing cholera. Inoculation before a religious fair in India.
Latrines and piped water were also provided for the pilgrims.
WHO photograph by Homer Page Cholera is an alarming disease and continues to attract more attention from public
health administrators and the general public than any other cause of diarrhoea. However,
it should be pointed out that most cases of cholera caused by the El Tor biotype of the
vibrio are mild, and that hospitalized cases constitute no more than 5 to 10 per cent of
all diarrhoea cases in endemic areas, except at times of epidemics. Even then, they are
treated and controlled in the same way as other acute diarrhoeas. Experience has shown
that specific strategies for cholera control are not effective, and consequently the
Technical Advisory Group of the WHO Diarrhoeal Diseases Control Programme, at its first
meeting in 1978, concluded that cholera control could best be achieved through national
programmes for the control of all diarrhoeal diseases.
|
 |
Guidelines for the control of cholera within the framework of national diarrhoeal
disease control programmes are available from: The Manager, Diarrhoeal Diseases Control
Programme, World Health Organization, 1211 Geneva 27, Switzerland. Dhiman Barua and Anne Martinez, Diarrhoeal Diseases Control Programme, World Health
Organization, Geneva, Switzerland.
(1) Mackay D 1979 Cholera research laboratory in Dacca, Bangladesh - a brief
history. Tropical Doctor, January pp 31-32.
(2) International Health Regulations (1969) Second annotated edition. Geneva, WHO
1974.
(3) WHO Weekly epidemiological record 1981 No 56: 97-98.
|
|
DDOnline
Diarrhoea Dialogue Online Issue 7 November 1981
3 Page 4 5
| Taking science where the diarrhoea is |
Finding the guilty organisms
David Candy looks at the key micro-organisms in
childhood diarrhoea and highlights recent advances in our understanding of this area. The last decade has been an exciting time for clinicians and scientists interested in
acute childhood diarrhoea. In addition to well-known microbial causes of human diarrhoea
(V. cholerae, Salmonellae, Shigellae and certain strains of E. coli) rotavirus,
Campylobacter and Yersinia are now recognized and our knowledge of the mechanisms involved
in E. coli diarrhoea has grown. Epidemiological studies have highlighted the
world-wide importance of rotavirus and E. coli diarrhoea and this review will
concentrate on these organisms. Rotavirus
Rotavirus causes perhaps 50 per cent of childhood diarrhoea increasing to 80 per cent
in temperate climates during winter. It was first identified in children in 1973 but had
previously been found in other young mammals. In young patients, watery diarrhoea preceded by vomiting should suggest rotavirus
infection. Dehydration occurs particularly rapidly because of vomiting and, although
recovery is usually uneventful with proper rehydration treatment, deaths do sometimes
occur. Although a proven cause of diarrhoea, rotavirus has been found in the stools of
healthy, newborn infants. Loss of electrolytes and water
Rotavirus is thought to cause diarrhoea by destruction of the cells lining the small
intestine. The cells replacing those shed into the gut lumen are less able to absorb
sugars. Unabsorbed sugar draws fluid from the rest of the body into the gut by osmosis. At
the same time, the process of sodium and water transfer, which depends on sugar absorption
in the upper gut, becomes less efficient. The overall effect is a huge loss of
electrolytes and water from within the small intestine which the large bowel is then
unable to reabsorb. The result is diarrhoea and further dehydration. E. coli
Only certain strains of E. coli cause diarrhoea in humans and these are
classified into three groups:
- Enterotoxigenic E. coli (ETEC)
These E. coli produce enterotoxins which stimulate the small intestine to secrete
electrolytes and water. Two enterotoxins of E. coli are recognized: a high
molecular weight protein readily destroyed by heating (heat-labile toxin (LT)
and a low molecular weight heat-stable toxin (ST).
- Enteroinvasive E. coli (EIEC)
EIEC invade the mucosa of the ileum and the colon, unlike ETEC
which remain on the mucosal surface.
- Enteropathogenic E. coli (EPEC)
EPEC do not produce either LT or ST,
neither do they invade the gut, yet they certainly cause diarrhoea. They have been
implicated by epidemiological means in outbreaks of diarrhoea in infants.
Serological classification
|
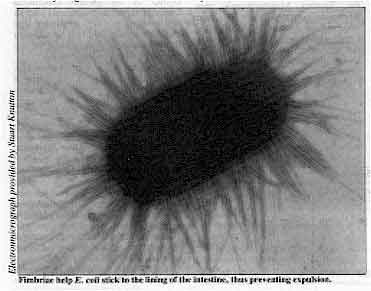
Fimbriae help E. coli stick to the lining of the
intestine, thus preventing expulsion. E. coli can also be classified serologically on the basis of a bacterial cell
wall antigen ('O' antigen). At present, 164 distinct 0 serogroups are
recognized. ETEC, EIEC and EPEC strains
tend to have distinctive O serogroups (see="#Table 1">Table 1).
However, E. coli possessing these O serogroups are not always
pathogenic and E. coli which have not been serotyped may also cause diarrhoea.
|
 |
Nevertheless, the serotyping of E. coli is a useful epidemiological tool as
other means of identifying potentially pathogenic E. coli are difficult, expensive
and not widely available.
| Table 1 |
O Serogroups in which ETEC, EIEC and EPEC
commonly occur |
| ETEC |
06, 08, 015, 020, 025, 078, 0115. 0148, 0159 |
| EIEC |
028, 0112, 0115, 0124, 0136, 0143, 0144, 0147, 0152 |
| EPEC |
055, 086, 0111, 0127, 0128, 0142 |
Infections
Infections with ETEC cause copious, watery diarrhoea and are an
important cause of warm season diarrhoea in young children in developing countries. EIEC produces fever, abdominal cramps, urgent and painful defaecation
(tenesmus) and watery diarrhoea, followed by scanty discharges of blood and mucus
(dysentery). Microscopic examination of methylene-blue stained faecal mucus shows pus and
red cells. EPEC can produce sudden cholera-like diarrhoea in adults whereas, in
infants. the disease often tends to be more prolonged with high mortality. It is possible
that these organisms produce uncharacterized enterotoxins. Another factor which may determine the ability of E. coli to cause diarrhoea is
whether they can produce hair-like structures called fimbriae or pili (2). These fimbriae
anchor E. coli to the lining of the small intestine, overcoming the attempts of the
bowel to expel them and allowing intestinal colonization.
|
|
DDOnline
Diarrhoea Dialogue Online Issue 7 November 1981
4 Page 5 6
| Taking science where the diarrhoea is |
V. cholerae
The vibrio associated with cholera was probably confined to the area around Calcutta
until 1813 when a series of pandemics occurred. Improved sanitation in industrialized
countries now keeps cholera at bay, but it is still endemic in parts of Asia (see="#page3">page three). Diarrhoea caused by cholera looks like rice water and a
litre or more of fluid can be lost every hour for several days. An enterotoxin almost
identical to LT is the cause of this symptom. Campylobacter
Campylobacter have been reported mainly from Europe, South Africa and North America
where as much as 15 per cent of infant diarrhoea may be due to this organism. Abdominal
pain, fever, diarrhoea and, occasionally, dysentery are the usual features. Pet dogs,
poultry and milk are likely sources of infection. Yersinia
Yersinia enterocolitica has been identified as a cause of gastroenteritis in
children in Canada, Europe, Japan and South Africa. It produces pain severe enough to
suggest a surgical emergency. Yersinia are invasive and also produce ST. Special
bacteriological techniques are needed to grow Yersinia and Campylobacter from stools.
During incubation, high temperatures favour Campylobacter and low temperatures encourage
Yersinia. Shigellae and Salmonellae
Shigellae are an important cause of diarrhoea in infants aged six months to two years.
Since shigellosis is spread by person-to-person contact, incidence is higher where
environmental health and personal hygiene are poor (3). As few as ten swallowed bacteria
are enough to cause the disease. Salmonellae are food-borne and contamination of animal carcasses in slaughterhouses is
the usual source. Symptoms resemble those produced by Campylobacter. Salmonellae and Shigellae are invasive and probably release toxins from inside the
intestinal cells. These cause secretion of fluid in the upper gut and cell damage in the
lower gut. Protozoal infections
Giardia lamblia and Entamoeba histolytica are single cell micro-organisms
(protozoa) which have been reported in most countries. G. lamblia grows in the
small intestine and is thought to be a cause of both acute and chronic diarrhoea, by
unknown mechanisms. E. histolytica prefers tropical zones and causes ulceration of
the large intestine. Other causes
Diarrhoea may be due to infections outside the gut, such as pneumonia, and this
possibility must be considered in any child with diarrhoea. Conclusions
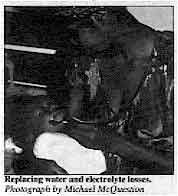
At present, the mainstay of treatment for acute diarrhoea is replacement of water and
electrolyte losses. Even in rotavirus infections, when sugar absorption is impaired, the
gut has sufficient reserves to allow successful treatment of diarrhoea by oral rehydration
with sugar and salt solutions. In future it may be possible to offer specific preventive measures or treatment for
specific causes of diarrhoea. Simple, low-cost methods for detecting the guilty organisms
will then be of great importance. Rotavirus can already be detected in stools by a test
relying on antibodies against the virus (enzyme-linked immunoabsorbent assay - ELISA)
which can be carried out without expensive equipment such as electron microscopes.
|
Replacing water
and electrolyte losses.
Photograph by Michael McQuestion The use of simpler tests in the field will mean that specific therapy is only given
when necessary (see="#page6">table on page six) and the use of antibiotics
prevented when contraindicated (e. g. rotavirus) or where such drugs may actually prolong
the illness (e. g. Salmonellae).
|
 |
Realizing these aims will depend on health workers being able to recognize the
causative organism early on in the disease. David Candy, Institute of Child Health, University of Birmingham.
(1) Rohde J E and Northrup R S 197.5 Taking science where the diarrhoea is. Acute
Diarrhoea in Childhood (Ciba Foundation Symposium 42): 339-366.
(2) Stickiness and sickness 1980. Diarrhoea Dialogue 2:3. '
(3) Khan M U 1980 Soap, water and shigellosis. Diarrhoea
Dialogue 2:3. Further reading: The most up to date review on all aspects of causes of acute diarrhoea is:
Infections
of the G. I. tract, Clinic in Gastroenterology, Vol 8 No 3 (1979). Ed. H P Lambert. W B
Saunder Co. Ltd., Eastbourne, UK. Especially chapters 1, 2, 3, 4, 5, 8 & 9.
For readers who would like further information David Candy has prepared a reading list
which is available free from AHRTAG. Please address your letter to the Executive Editor,
Diarrhoea Dialogue, AHRTAG. 85 Marylebone High Street, London W1M 3DE, UK.
|
|
DDOnline
D iarrhoea Dialogue Online Issue 7 November 1981
5 Page 6 7
CLINICIAN'S GUIDE TO AETIOLOGY
This table gives the information that will help to identify, on clinical grounds alone,
the most common agents of diarrhoea. It is greatly simplified. For example, some agents
produce a variety of clinical features. Only agents of major importance world-wide have
been included. In certain areas, at certain times, the picture may be quite different. Try
and find out what the important causes of diarrhoea are in your area. Caution: There are a number of other conditions associated with diarrhoea such
as infections outside the gut (e.g. measles and malaria), malnutrition, food intolerance
etc. Remember to look for these and give specific treatment where appropriate. If readers find this table useful, we may present other information in the same way
in future issues of Diarrhoea Dialogue. Please send us your comments on this
clinician's guide.
|
| COMPLAINT |
ASSOCIATED CLINICAL FEATURES |
INCUBATION PERIOD |
EPIDEMIOLOGICAL FEATURES |
ORGANISMS |
FIRST LINE TREATMENT |
| COMMON |
OTHERS |
ACUTE WATERY DIARRHOEA

The stool takes the shape of the container |
Vomiting
Fever |
Severe dehydration in some |
24-72 hours |
Infants and young children
Common
world-wide in all socio-economic groups
Peak in colder seasons in temperate climates |
Rotavirus |
Rehydration therapy |
Nausea
Vomiting
Abdominal pain
|
Fever
Malaise
Severe dehydration |
6-72 hours |
Infants and young children in developing countries
Travellers
diarrhoea in adults |
Enterotoxigenic Escherichia coli (ETEC) |
Rehydration therapy |
Nausea
Vomiting
Fever
Chills
Abdominal pain |
Malaise |
8-36 hours |
Children
Common world-wide
Food-borne outbreaks (animal products)
Warmer seasons |
Non-typhoid Salmonellae |
Rehydration therapy |
Abdominal pain
Fever
Malaise |
Chills
Blood and pus in the stools |
3-5 days |
World-wide distribution
In developed
countries may be food-borne (animal products) or transmitted by handling of animals |
Campylobacter |
Rehydration therapy Erythromycin
in severe cases |
Vomiting
Abdominal pain |
Severe dehydration
Circulatory
collapse, 'shock' |
1-3 days |
Children in endemic areas
Adults in
newly affected areas
Not found in Latin America |
Vibrio cholerae |
Rehydration therapy Tetracycline |
Nausea
Vomiting |
Fever |
6-72 hours |
Nursery outbreaks in developed countries
Uncertain
in developing countries |
Enteropathogenic Escherichia coli (EPEC) |
Rehydration therapy |
DYSENTERY
The stool is soft and watery with blood and/or pus |
Fever
Abdominal pain |
Malaise
Vomiting
Urgency to defaecate
Painful spasm on defaecation |
36-72 hours |
Children
Poor hygiene
Malnutrition
Institutions
Warmer seasons |
Shigellae |
Rehydration therapy Ampicillin or
Trimethoprim - Sulfamethoxazole |
PROLONGED DIARRHOEA (OR DYSENTERY)
For at least 7 days, stools have been more frequent or of softer
consistency (with or without blood or pus) |
Abdominal discomfort |
|
2-6 weeks |
A11 age groups
World-wide
distribution |
Entamoeba* histolytica |
Metronidazole |
Abdominal distension
Flatulence |
Anorexia
Nausea
Malabsorption
Frothy stools |
1-3 weeks |
Young children
Some travellers
Poor hygiene
World-wide distribution |
Giardia*
lamblia |
Metronidazole |
* Can be identified on examination of the stools
with a light microscope.
Blood and pus from Shigellae and Campylobacter can also be
identified. |
Produced in collaboration with the Ross Institute
of the London School of
Hygiene and Tropical Medicine and The Save the Children Fund. |
|
DDOnline
Diarrhoea Dialogue Online Issue 7 November 1981
6 Page 7 8
Costa Rica
The highly successful Costa Rican experience with oral rehydration therapy has
been shared with several other Latin American countries. Since a trial oral rehydration (OR) project was begun in Costa Rica at the beginning of
1978, ORT has proved an effective life-saver in both bacterial and rotaviral infant
diarrhoea, including neonates (1 & 2). Routine implementation of OR in the National
Children's Hospital has resulted in more than an 80 per cent reduction in mortality. The
technique is easily understood both by health personnel and mothers visiting the emergency
unit at the hospital (3). In addition, health centres in both urban areas and the
countryside have also been able to introduce oral rehydration therapy. Field project
|
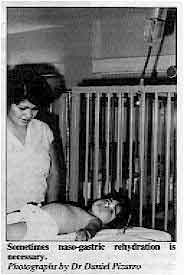
Sometimes
naso-gastric rehydration is necessary.
Photographs by Dr Daniel Pizarro A field project to monitor oral rehydration therapy given by mothers to their children
in rural areas was started by the Instituto de Investigaciones en Salud (INISA) in 1980.
Mothers soon learned the technique and treated children successfully. At the same time,
comprehensive teaching material for health personnel was prepared by the state welfare
system, while the Ministry of Health established a national programme of diarrhoeal
disease control with technical assistance from the Pan American Health Organization
(PAHO).
|
 |
Sharing experiences
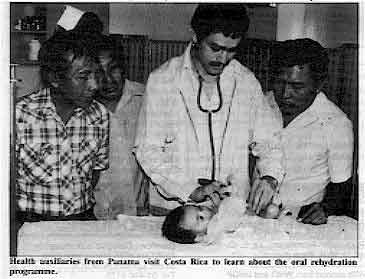 |
Health auxiliaries from Panama visit Costa Rica to learn about
the oral rehydration programme.
During the past three years, the Costa Rican experience has been shared with several
Latin American countries. Health personnel from Bolivia, El Salvador, Guatemala, Honduras,
Panama, Paraguay and Venezuela visited Costa Rica for a first-hand view of the OR
programme. Visiting doctors spent a week in the emergency unit of the National Children's
Hospital, INISA's rural programme in Puriscal, the rural hospital in Grecia and the
Department of Maternal and Child Health at the health ministry.
|
Mortality rates drop
Since 1978, about 15,000 dehydrated children (including 160 neonates) have been
rehydrated in the emergency unit of the National Children's Hospital. Mothers have been
taught about the causes, transmission and management of diarrhoea as well as techniques to
rehydrate and prevent dehydration among infants. All these efforts have had a considerable
impact on both hospital mortality rates and overall diarrhoeal disease mortality in Costa
Rica (4). Daniel Pizarro, Emergency Service, 1 National Children's Hospital, San Jose, Costa
Rica.
(1) Nalin D R et al 1979 Oral rehydration and maintenance of children with
rotavirus and bacterial diarrhoeas. Bulletin of the World Health Organization vol
57: 453-459.
(2) Pizarro D et al 1979 Evaluation of oral therapy for infant diarrhoea in an
emergency room setting; the acute episode as an opportunity for instructing mothers in
home treatment. Bulletin of the World Health Organization vol 57: 983-986.
(3) Pizarro D et al 1979 Oral rehydration of neonates with dehydrating diarrhoeas.
The Lancet, vol 2: 1209-1210.
(4) Mata L J 1981 Diarrhoeal diseases. How Costa Rica won. World Health Forum, 2:
141-142.
|
|
DDOnline
Diarrhoea Dialogue Online Issue 7 November 1981
7 Page 8
Ethiopia: too few medical workers
I am the Director of an orphanage in a rural part of Ethiopia. In the orphanage there
are children between seven to fourteen years old. They are from the drought stricken area.
I have found your issues of Diarrhoea Dialogue very helpful since I am not
medically trained and there is also a scarcity of medical workers in my country. I am
interested in receiving future issues. Birhanu T Michael, P. O. Box 545, Dessi/Wollo, Ethiopia.
Lack of one litre bottles In the nutrition centres in the Salvadorean refugee camps in Honduras we started oral
rehydration programmes for children with diarrhoea. The oral rehydration solution is
prepared daily for those malnourished children with diarrhoea. In addition to using the
available packets of oral rehydration salts, the nutrition workers teach the mothers how
to prepare the home-made solution. When the programme started in August, other mothers in
the camps began bringing their children who had diarrhoea to the nutrition centres to
receive the oral rehydration solution even though they receive the packets at the health
centres.
|
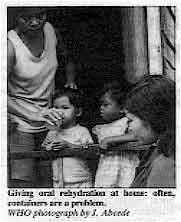
Giving oral rehydration at home: often, containers are a problem.
WHO photograph by J. Abcede The mothers told us that the problem with the packets is that they do not have
containers in which to measure or store one litre of rehydration solution. Since we
prepared the solution in the nutrition centre and the mothers would bring whatever
containers they had, such as ½ litre bottles or ¼ litre glasses which we would refill as
needed, children with diarrhoea began receiving the oral rehydration solution.
|
 |
The shortage of one litre containers appears to be very common and one idea to help
resolve it would be to make the oral rehydration packets with four sub-sections, each
containing the correct amount of salts for a ¼ litre glass - a container most mothers
have in their homes. I am interested in learning whether such packets have been
manufactured and at what cost in comparison to the others. I would also recommend that
UNICEF consider developing such packets so that more mothers could prepare the oral
rehydration solution in their homes for their children with diarrhoea. Solange T Muller, Apartado A-51, Managua, Nicaragua.
Editors' note: A number of readers from as far apart as Kiribati in the Pacific to the Ivory Coast
in West Africa, have commented on the value of naso-gastric feeding for rehydration in
diarrhoea. In some cultures, this procedure is associated with feeding unconscious
patients, and parents have become worried because they associate the technique with
impending death. However, in cases of severe diarrhoea, where the child is vomiting,
naso-gastric feeding can be a life-saver and an excellent means of showing how effective
the techniques can be.
Naso-gastric feeding in Kiribati ...
Ms J. Aitken's letter (Diarrhoea Dialogue 6) prompts us
to write concerning our experience with nasogastric administration of oral rehydration
(OR) fluids in childhood diarrhoea. Like her, we find this an extremely useful method in
children whose diarrhoea is accompanied by vomiting, where frequently the mother is
reluctant to give fluids by mouth because it provokes vomiting. Supplies to these small coral atolls are precarious and frequently sugar, salt and OR
packets are unavailable. So we use water from unripe (drinking) coconuts with an added
tablespoon (for each nut) of sugar or honey, if available, or a local syrup (kamaimai)
prepared from the sap of the coconut blossom. This mixture is equally effective by spoon
or nasogastric drip, but in the latter case it needs to be filtered before use since
fragments of the unripe coconut flesh tend to block the tube. For those unfamiliar with techniques of naso-gastric rehydration, details are given in
Dr Maurice King's book Primary Child Care: a manual for health workers Vol 1 1980
(reprinted), available from Oxford University Press, Oxford OX2 6DP, UK. Dr Antony Franks (District Medical Officer) and Miss Baane Timi (Public Health
Nurse), Abemama Atoll, Kiribati, Central Pacific.
... and Afghanistan
The naso-gastric method has been used successfully for the rehydration of babies, who
refuse to drink fluids or in whom even small amounts cause vomiting, in one of the MCH
centres (Shewaki) near Kabul for over three years. Health workers are taught how to insert
a naso-gastric tube and how to make sure it is in the stomach before starting the drip.
This method has also been included in the training material for health workers in
Afghanistan. Dr Shanti Ghosh, WHO Medical Officer on Family Health Services Development,
Afghanistan.
|
Scientific editors Dr Katherine Elliott and Dr William Cutting
Executive editor Denise Ayres Editorial advisory group
Professor David Candy (UK)
Dr I Dogramaci (Turkey)
Professor Richard Feachem (UK)
Dr Michael Gracey (Australia)
Dr Norbert Hirschhorn (USA)
Dr D Mahalanabis (India)
Professor Leonardo Mata (Costa Rica)
Dr Mujibur Rahaman (Bangladesh)
Dr Jon Rohde (USA)
Ms E O Sullesta (Philippines)
Dr Paul Vesin (France)
Dr M K Were (Kenya) With support from WHO and UNDP
|
Issue no. 7 November 1981
Page Navigation
This edition of Dialogue on Diarrhoea Online is produced by Rehydration Project. Dialogue on Diarrhoea was published four times a year in English, Chinese, French, Portuguese, Spanish, Tamil,
English/Urdu and Vietnamese and reached more than a quarter of a million readers worldwide. The English edition of Dialogue on Diarrhoea was produced and distributed by Healthlink Worldwide. Healthlink Worldwide is committed to strengthening primary health care and
community-based rehabilitation in the South by maximising the use and impact
of information, providing training and resources, and actively supporting
the capacity building of partner organisations. - ISSN 0950-0235 Reproducing articles
Healthlink Worldwide encourages the reproduction of
articles in this newsletter for non-profit making and educational uses. Please
clearly credit Healthlink Worldwide as the source and, if possible, send us a copy of any uses made of the material.
|
updated: 23 August, 2019
updated: 23 August, 2019
|






