|
| |
Issue no. 6 - August 1981
pdf
 version of this Issue version of this Issue
|
There is much information in this issue that is valuable
and useful. Online readers are reminded, however, that treatment guidelines and health
care practices change over time. If you are in doubt, please refer to
WHO's up-to-date Dehydration Treatment
Plans.
|
updated: 23 April, 2014
Pages 1-8 Diarrhoea Dialogue Online Issue 6 -
August 1981
|
DDOnline
Diarrhoea Dialogue Online Issue 6 August 1981
 Page 1 2
Page 1 2
Diarrhoea and child growth
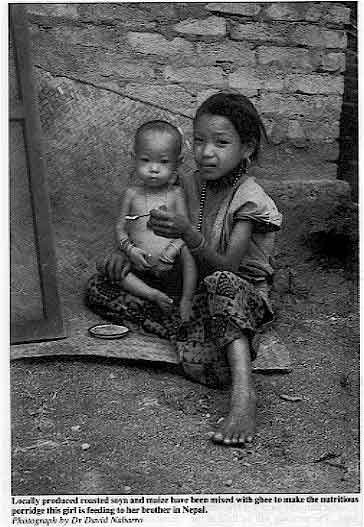 |
Locally produced roasted soya and maize have been mixed with
ghee to make the nutritious porridge this girl is feeding to her brother in Nepal.
Photograph by Dr David Nabarro In healthy children, the nutritional consequences of diarrhoea are not significant.
However, diarrhoea can be critical for malnourished children as it causes the appetite to
drop and the gut becomes less able to absorb nutrients. Rehydration is obviously the priority when a child has diarrhoea. Oral rehydration
fluid not only helps to relieve dehydration but also has a positive long-term effect on
the nutritional status of the child. Studies in the Philippines and Turkey have shown that
children treated with oral rehydration fluid continued to gain more weight for the next
six months (in comparison to a control group) (1). However, some children will not accept
sugar-salt solution easily and a useful alternative to this in the early stages of
diarrhoea is rice water (see="#page2">page two).
|
- Children with diarrhoea should be encouraged to feed as soon as possible during an
attack. They should not be starved. Even though food passes through the digestive
tract much more rapidly during diarrhoea, a certain amount of nutrients are still
absorbed. Breastfeeding should always continue.
- High energy foods such as fats, potatoes and yoghurt are well absorbed during diarrhoea
(page six). It should be possible to feed the child if you use a cup
and spoon and give small amounts frequently.
- If possible, the child should receive an extra meal a day for the first week after the
attack.
(1) Azurin et al 1977 A positive effect on the nutrition of Philippine
children of an oral glucose-electrolyte solution given at home for the treatment of
diarrhoea. Bulletin of the World Health Organization vol 55.
|
In this issue...
- Mike Rowland reports on infant nutrition and diarrhoea in The Gambia
- Persuading children with diarrhoea to eat
- News and reviews
|
|
DDOnline
Diarrhoea Dialogue Online Issue 6 August 1981
1 Page 2 3
Rice water and diarrhoea
|
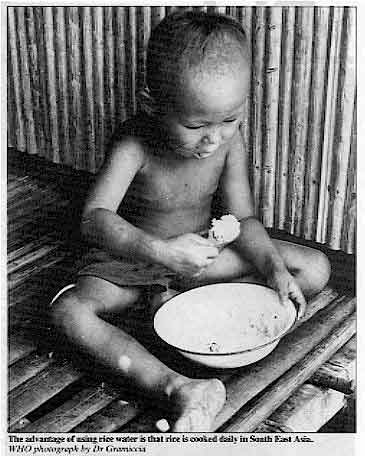
The advantage of using rice water is that rice is cooked daily
in South East Asia.
WHO photograph by Dr Gramiccia In South East Asia, rice is prepared in two ways - to produce either dry, cooked rice
or, with extra water, rice porridge. This leaves a fluid (rice water) on top of the cooked
rice grains. Professor Wong Hock Boon, a paediatrician working in Singapore, has been using rice
water to rehydrate babies for several years. If the babies are bottle-fed rice water is
given exclusively for the first 24 hours of treatment - breastfeeding can continue as
normal (1). Professor Wong and his colleagues have found that many babies who have not
responded to other rehydration solutions respond well to rice water. If diarrhoea starts
again with the re-introduction of milk, extra rice water is given with additional rice
porridge. Older babies are sometimes given rice porridge alone.
|
 |
The means by which rice water helps to stop diarrhoea are still being researched. One
explanation could be that starch-like sugars tend to draw less fluid out of the body and
into the gut compared with a similar amount of simple sugar such as glucose. Some babies
with diarrhoea can digest starch more easily than simple sugars. The International Centre
for Diarrhoeal Disease Research, Bangladesh (ICDDR, B) is carrying out studies on the
inclusion of locally available starches (such as rice starch) as the carbohydrate in oral
rehydration solution. As Professor Wong stresses, the advantage of using rice water is that rice is cooked
daily in South East Asia. The rice water is boiled and does not have to be made up and
kept in large quantities as is frequently the case with sugar-salt rehydration solutions. If you would like more information about the use of rice water for rehydration, write
to: Professor Wong Hock Boon, National University of Singapore, University Department of
Paediatrics, Singapore General Hospital, Outram Road, Singapore. For information on ICDDR, B's work on locally available starches, write to: Library and
Publication Unit, International Centre for Diarrhoeal Disease Research, Bangladesh, G.P.O.
Box 128, Dacca-2, Bangladesh. (1) Wong H B 1981 Rice water in treatment of infantile gastroenteritis. The Lancet
vol 2: 102-103.
Bangkok seminar
A seminar on diarrhoeal diseases of children in South East Asia in the context of
primary health care will take place in Bangkok from 9-12 November 1981. The meeting will
be held at the Faculty of Tropical Medicine, Mahidol University, Bangkok. It is being
jointly organized by the SEAMEO Regional Tropical Medicine and Public Health Project, the
Faculty of Tropical Medicine, Mahidol University, and the Gastroenterology section of the
Paediatric Society of Thailand. For further details, write to: Dr Tan Chongsuphajaisiddhi,
Faculty of Tropical Medicine, Mahidol University, 420/6 Rajvithi Road, Bangkok 4,
Thailand. Cable TROPMED. Tel. 2819224, 2819234. IRC newsletter
The International Reference Centre for Community Water Supply and Sanitation has asked
us to mention their monthly newsletter which looks at all aspects of water supply and
sanitation. The publication is free and available in either English or French from:
International Reference Centre for Community Water Supply and Sanitation, P.O. Box 5500.
2280 HM Rijswijk, The Netherlands.
|
|
DDOnline
Diarrhoea Dialogue Online Issue 6 August 1981
2 Page 3 4
Diarrhée Dialogue
|
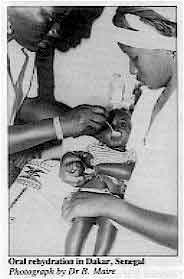
Oral rehydration in Dakar, Senegal
Photograph by Dr B. Maire Diarrhoea Dialogue is now available in French. It is being produced and
distributed with the help of the Organisme de Recherches sur l'Alimentation et la
Nutrition Africaine (ORANA) and the Association Africaine d'Education pour le
Developpement (ASAFED) in Dakar, Senegal. We have sent copies of the first edition to
readers currently on our mailing list in French-speaking countries. However, if you have
not yet received a copy and would like to be on the French mailing list please contact us.
|
 |
UNESCO prize Readers may be interested to know that our Costa Rican editorial adviser, Dr Leonardo
Mata, and his team have been awarded the UNESCO Science Prize for 1980 for their
outstanding contribution to scientific and technological development in developing
countries. Erratum In the article on pit latrines in Mozambique (Diarrhoea
Dialogue 5,="dd05.htm#page3">Diarrhoea
Dialogue 5, page 3) there was a mistake in the sentence beginning "The
slightly conical shape makes it possible to eliminate the steel reinforcement on a slab
1.1 metres in diameter and less than 4 cm thick." The concrete slab should in fact be
1.5 metres in diameter. The large diameter allows the load to be carried far from
the edge of the pit in unstable sandy soils, as well as permitting a wider lined pit in
areas with high water tables. Reviews
Sanitation without Water
Uno Winblad and Wen Kilama
133 PP
Swedish International Development Authority (SIDA) Free This is a useful manual first published in 1978 and recently re-issued in a revised
form. It describes composting latrines and improved pit latrines of various kinds. The
information is of particular interest to health officers, sanitarians and medical
auxiliaries working in rural areas. The illustrations in the manual are particularly good. Requests for copies to: Swedish International Development Authority (SIDA), S-105 25
Stockholm, Sweden. Rural Water Supply in Developing Countries
Proceedings of a workshop on training held in Zomba, Malawi, 5-12 August 1980
144 pp Sanitation in Developing Countries
Proceedings of a workshop on training held in Lobatse, Botswana, 14-20 August 1980
172 PP In August 1980, two regional workshops were organized by the International Development
Research Centre (IDRC) - one, in Malawi, on water supply and another, in Botswana, on
sanitation. The aim of the workshops was to help spread information on low-cost
technologies and to discuss curricula changes and training. These well-presented
proceedings include papers given at the workshops, descriptions of field visits and action
plans. The books are free and IDRC hopes that, through wide dissemination, the influence
of the workshops can spread beyond the countries of the attending delegates. Requests for copies to: International Development Research Centre
(IDRC), Box 8500,
Ottawa, Canada K1G 3H9.
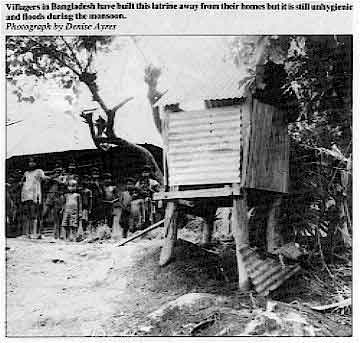 |
Villagers in Bangladesh have built this latrine away from their
homes but it is still unhygienic and floods during the monsoon.
Photograph by Denise Ayres
|
|
|
DDOnline
Diarrhoea Dialogue Online Issue 6 August 1981
3 Page 4 5
| Diarrhoeal disease and nutrition in childhood |
The diarrhoea-malnutrition complex
The main mechanism by which diarrhoea leads to malnutrition is uncertain and few
data exist to clarify the situation. Mike Rowland reports from a
long-term study in The Gambia looking into this problem. Diarrhoea and malnutrition are major causes of childhood morbidity and mortality in
less-developed countries. The interaction between the two was highlighted during the early
1960's and an excellent account later published (1). The complex relationship is still not
fully understood but two generalizations appear valid. Failure to thrive
Malnourished children (i.e. children who are failing to thrive) appear to suffer more
severe episodes of diarrhoea than their better nourished counterparts (2) and to excrete
infective organisms for longer. This situation is complicated by the fact that impaired
growth in many of these children may be largely due to the heavy burden of diarrhoea
already experienced. Diarrhoea more than any other infection causes serious growth-faltering in children in
many areas of the world. It is significant that in the three continents where this
has been well described all mothers in the study communities breastfed their children for
long periods. The children would almost certainly have been worse off if fed otherwise but
protection is not complete in most subjects (3) nor does breastfeeding preclude serious
morbidity in under-privileged communities. Food shortage
Some workers feel that food shortage in the community plays a relatively minor role in
early childhood growth-faltering and that if diarrhoea could be prevented near-normal
growth could occur. The main mechanism by which diarrhoea leads to malnutrition is
uncertain and few data exist to clarify the situation. Some suggest that anorexia is the
main cause, others that malabsorption due to abnormalities of gut flora and function is a
more likely explanation. Seasonal variation
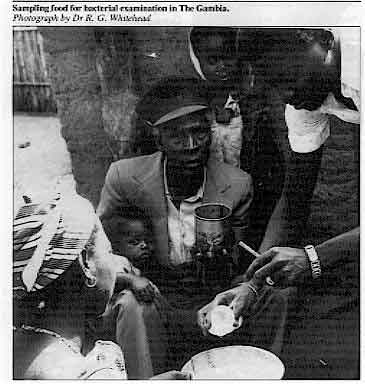 |
Sampling
food for bacterial examination in The Gambia.
Photograph by Dr R. G. Whitehead In The Gambia there is marked seasonal variation in growth and disease in young
children and studies there (4) have thrown some light on these problems. At certain times of the year it appears that normal and even catch-up growth is
possible on a traditional diet of locally grown food, provided the individual child
suffers little diarrhoea. At other times of the year, however, growth is uniformly
depressed whether or not diarrhoea occurs and this tends to be the case in the traditional
"hungry season". Thus diarrhoea at different times appears to have an effect on
growth of widely differing magnitude (5). Just as the aetiology may vary from season to
season and also from one age-group to another, so may the nature and severity of the
pathological processes which follow infection.
|
Malabsorption In the Gambian community studied diarrhoea is certainly responsible for some reduction
in complementary food intake in the weanling child (i.e. the child receiving both breast
milk and additional foods), but so are a number of other infections which have little or
no detectable effect on growth. Furthermore there are indirect indications that
some degree of intestinal malabsorption may be common in the young village children. On
balance it appears that in this community at any rate malabsorption is more important than
anorexia in explaining diarrhoea-induced growth-faltering (6).
|
|
DDOnline
Diarrhoea Dialogue Online Issue 6 August 1981
4 Page 5 6
| Diarrhoeal disease and nutrition in childhood |
Weanlings at risk
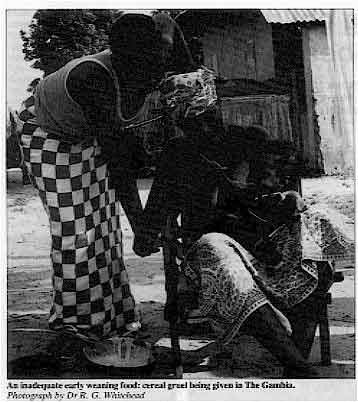 |
An inadequate early weaning food: cereal gruel being given in
The Gambia.
Photograph by Dr R. G. Whitehead Whatever the mechanism it seems clear that the initiation of the weaning process, even
when breastfeeding is continued for long periods afterwards, puts children seriously at
risk. This is supported by examination of the weaning foods used. In The Gambia the
earliest weaning foods are cereal gruels or paps. These are grossly inadequate
nutritionally with approximately half the energy-density of breast milk and many of the
other nutrients are inadequate or totally lacking. Furthermore it is these earliest foods
which show the highest levels of bacterial contamination, both with faecal
"marker" organisms and known gut pathogens (7). Local fuel shortages make it
impossible for mothers to cook frequent meals for small children. Instead larger
quantities are prepared and kept for long periods, when they may easily become
contaminated.
|
A total approach In this situation we cannot afford to neglect any health strategy including promotion
and active support of the breastfeeding mother, the appropriately timed introduction of
hygienically prepared, nutritious weaning foods, the general use of complete oral
rehydration mixtures, and various aspects of environmental sanitation. In the course of
treating children with diarrhoea breastfeeding should be maintained and other foods
withheld only if there appears to be clinically important intolerance (and not just
malabsorption) to these foods. We may hope for vaccines against a number of diarrhoeal agents in the near future but
as little is known of the impact of the various individual agents on growth in different
communities it would be unwise to try to predict the efficacy of these measures. What it
would be helpful to know at this stage is which, if any, organisms are particularly
important in the diarrhoea-malnutrition complex; useful work is already being undertaken
along these lines in Bangladesh (8). Mike Rowland, Medical Research Council, Fajara, The Gambia, West Africa. (1) Scrimshaw N S et al Weanling diarrhoea - a synergism of infection and
nutrition. Interactions of nutrition and infection. WHO Monogram Ser. No 57: 216-261
(2) Tomkins A M 1981 Nutritional status and severity of diarrhoea among pre-school
children in rural Nigeria. The Lancet, April 18 : 860-862
(3) Rowland M G M et al 1980 Bacteriostasis of Escherichia coli by milk. VI. The in-vitro
bacteriostatic property of Gambian mothers' breast milk in relation to the in-vivo
protection of their infants against diarrhoeal disease. Journal of Hygiene Cambridge 1980
85: 405-413
(4) Rowland M G M, Whitehead R G 1978 The epidemiology of protein-energy
malnutrition in children in a West African village community. Medical Research Council.
Available from Nutrition Planning.
(5) Rowland M G M et al 1977A quantitative study into the role of infection in
determining nutritional status in Gambian village children. British Journal of Nutrition
1977 37:441-450
(6) Rowland M G M 1980 (in press) Interaction between diarrhoea and malnutrition:
aetiological considerations. In: Acute enteric infections in children. New prospects for
treatment and prevention. Proceedings of Nobel Conference 3.
(7) Rowland M G M et al 1978 Bacterial contamination in traditional Gambian weaning
foods. The Lancet January 21: 136-138
(8) Black R E 1980 (in press) Epidemiological importance of diarrhoeal agents in
Bangladesh. In: Acute enteric infections in children. New prospects for treatment and
prevention. Proceedings of Nobel Conference 3.
|
|
DDOnline
Diarrhoea Dialogue Online Issue 6 August 1981
. 5 Page 6 7
Persuading children with diarrhoea to eat
Encouraging a child with diarrhoea to eat is a difficult and exhausting task for
the mother. However, children should be encouraged to eat as early as possible during an
attack.
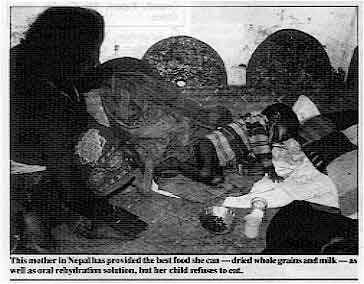 |
This mother in Nepal has provided the best food she can - dried
whole grains and milk - as well as oral rehydration solution, but her child refuses to
eat.
Photographs by Dr David Nabarro Although rehydration is the most immediate and vital aspect of the management of
diarrhoea, the giving of energy in some form of food is essential. In many parts of the
world, people think it is necessary to starve children with diarrhoea. This is dangerous.
Starving can start off malnutrition, or worsen it, making the child too weak to fight
infection.
|
Extra meal Food should be given to the child as soon as dehydration is corrected, any vomiting
stops, and the appetite returns. Breast milk and other liquids (but not cows milk and
infant formula foods) should continue during oral rehydration. Once the diarrhoea has
stopped, at least one extra meal should be given each day for a week if possible. Small portions Feed the child with small portions throughout the day. Do not force him to take too
much food at a time. The composition of the food can be changed gradually until the child
goes back to his normal solid diet. The mother will know which food the child likes best
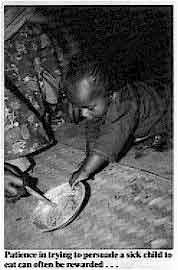
and can further encourage his appetite by adding additional flavouring. Patience in trying to persuade a sick child to eat can often
be rewarded
|
Every effort should be made to feed the child as there is evidence that even during
diarrhoea as much as 60 per cent of nutrients are absorbed. In many developing countries,
low-energy gruels form the basis of children's diets, and therefore the sick child has to
eat much more to obtain sufficient calorie intakes. Try to give a child with diarrhoea a
higher intake of energy foods (see="#CHART A">Chart A). Mothers need to be
shown how to use locally available foods to the best advantage for their children. |
 |
Other important points
- Try to prepare all food in a clean place, using clean pots and utensils.
- Food should be eaten soon after it is cooked. If not, it should be thoroughly heated
again before eating.
- Wash uncooked food in clean water before eating.
- To be sure a young child is getting enough food, try to give him a separate plate or
dish. The dish should have a cover.
|
CHART A.
Which foods to give:-During diarrhoea foods which contain a lot of
fibre (e.g. coarse fruits and vegetables, vegetable and fruit peel and whole-grain
cereals) and spicy foods should be avoided. Energy-rich foods are important (such as
bananas, potatoes, yoghurt and cereals cooked with milk, sugar and a little oil) and foods
containing potassium (e. g. pineapple and citrus fruits and their juices, bananas and
coconut milk) can also be given. |
|
DDOnline
Diarrhoea Dialogue Online Issue 6 August 1981
6 Page 7 8
From: Sigrid Woelke, Santa Cruz, Bolivia I am a nutritionist working in a poor rural area in Bolivia where there is a lot of
childhood diarrhoea. It seems an excellent idea to me to publish a newsletter about this
widespread and dangerous disease.
- In issue three, page two, you mention the dangers of giving the wrong quantities
of oral rehydration solution. What are these dangers? Do they also apply to homemade
solutions or just for the packages of sugar and salt?
- Some literature includes sodium bicarbonate when suggesting recipes for homemade
oral rehydration solution, and from articles in Diarrhoea Dialogue I gathered that the
packaged oral rehydration salts include sodium bicarbonate as well. However, in issue
three all the homemade versions seem to leave it out and use only sugar and salt. Isn't
the sodium bicarbonate important for treating acidosis in diarrhoea?
- I would like to get some recipes for oral rehydration solution that would be
useful in areas where there is no possibility of taking children to the doctor. We have no
sachets of oral rehydration salts because the idea of oral rehydration is still very new
here.
Table A indicates how much fluid should be given
according to the weight of the child. As far as composition is concerned, there are fewer
problems with adding too much sugar to the quantity of liquid used - although this can
happen in some cases. It is far more likely that when making up homemade oral rehydration solution, too much
salt will be added causing hypernatraemia. Again, you can avoid this by measuring out the
salt carefully and by tasting the solution. It should not taste saltier than tears. If you
are using water from a salty spring source, you should add slightly less salt to the
solution. If you are using sachets of oral rehydration salts, as long as the contents are
mixed with the correct amount of liquid specified, there should not be a problem of over
or under concentration. As far as sodium bicarbonate is concerned, add this to homemade oral rehydration
solution if it is locally available. If not, don't worry, the most important elements of
the solution are the sugar, salt and water. Homemade solutions
There are various ways of making up homemade solutions.
- You can measure out one heaped 5ml teaspoonful of sugar and a finger pinch of salt. Add
this to about 250cc of water. It is a good idea to make up the solution in quantities as
small as this so that you can use it quickly and avoid storing it for long periods. The
UNICEF sachets provide enough salts for one litre of solution, but many sachets being
locally produced are designed for smaller quantities. For example, in Costa Rica the
Instituto de Investigaciones en Salud has developed a pack of oral rehydration salts -
Sueroral - which is being widely distributed together with instructional materials for
health workers and mothers. The pack contains the correct amount of salts to be mixed with
8 oz of water (Diarrhoea Dialogue 3, page 3).
- You can obtain two-ended plastic spoons from TALC (Teaching Aids at Low Cost, 30
Guilford Street, London WC1N 1EH, United Kingdom) to measure out enough salt and sugar for
200cc of water. The TALC spoons are available with instructions printed on in different
languages and all carry the advice that the oral rehydration solution should be tasted
before it is given to the child and not used if it tastes saltier than tears.
Homemade formulae do not include any form of potassium replacement. There are, however,
many locally available sources of potassium that can be added to the solution (such as
bananas, oranges and lemons. See="dd03.htm#page7">Diarrhoea Dialogue 3, page
seven and Diarrhoea Dialogue 5, page seven). Clear instructions
With all methods of making up oral rehydration solution, mothers and health workers
must be given clear instructions on how to prepare the solution correctly. This was well
illustrated in an interesting study carried out in Honduras. The authors looked for a
simple method of preparing sugar-salt solution using measuring utensils most often
available in developing countries (1). Village mothers were asked to bring a teaspoon and
a one litre container to the health centre. Sugar and salt were bought in a town market.
The method of preparation (one level 5ml teaspoon of salt and four heaped teaspoons of
sugar in a litre of water) was described to a 15-year-old girl who was training as an
assistant health auxiliary. Sixteen of the mothers brought the correct size of teaspoon, three brought smaller
teaspoons and one a 20ml tablespoon. The solutions made up by the mothers ranged in sodium
level from 60-145mmol/l and in sucrose from 1.3-3.7g per cent, all within a safe and
effective range. The authors of the study stress the importance of one person in a village being taught
to discern the correct size of utensils so that she can teach and supervise preparation of
oral rehydration solutions by mothers. Often, the village midwife can serve this function.
(1) Levine M M el al 1981 A practical, reliable method for preparing simple
sugar/salt oral rehydration solution. The Journal of Tropical Medicine and Hygiene, 84:
73-76.
|
Table A
How much oral rehydration solution to give |
| Child' s weight in kilograms |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
10 |
11 |
12 |
13 |
14 |
15 |
20 |
30 |
40 |
50 |
For the first 4-6 hours of dehydration give:
All measurements in ml. |
200-400 |
400-600 |
600-800 |
800-1000 |
1200 |
1500 |
2500 |
3500 |
4500 |
| For continuing diarrhoea and to prevent dehydration from coming
back use Method 1 or 2 |
Method 1: After every diarrhoea stool give: |
50 |
100 |
150 |
200 |
300 |
350 |
400 |
| Method 2: Over 24 hours give: |
400 |
600 |
800 |
1000 |
2500 |
Reproduced from Diarrhoea Dialogue 3, November 1980
|
DDOnline
Diarrhoea Dialogue Online Issue 6 August 1981
7 Page 8
Urban water supplies
UNICEF in Lagos has been kind enough to send me a copy of Diarrhoea
Dialogue 4. Such a newsletter is long overdue. Although many developing
countries, including Nigeria, are trying to have clean pipe-borne water within the next
decade the concentration is more in the urban centres. Eighty per cent of African people are rural dwellers. They depend upon the shallow
wells, suspicious water flowing from one village to the other and dirty stagnant pools
near the farm tents. They die in thousands of water-borne diseases. Most of the pipes imported from the advanced nations are not durable. Africa has big
rivers, good falls and heavy rainfall. Yet we suffer from inadequate water supplies in big
cities. There is poor planning by most African governments and poor equipment supplied from
Europe. Both the suppliers and the users are guilty. Unless there is a change of heart on
both sides we may not achieve so much in many African countries by the year 1990. Ade Adetona, P. O. Box 6924, Marina St, Lagos, Nigeria.
Naso-gastric drip
We are a doctor and nurse working in a very poor and neglected area in Bihar,
north-east India. Our main work is the training of village health workers. We make up our
own rehydration mixture in plastic bags and the cost of each works out at about 35 paise
whereas electrolyte packets available in the shops cost at least 15 times as much. We have found that in cases of babies with diarrhoea and vomiting and severe
dehydration where even small spoonfuls of fluid lead to vomiting, a naso-gastric drip is
very effective. We have not heard of this method being used before and would like to hear
about any similar experiences. Ms Janet E. Aitken, c/o Bimalendu Das, P. O. Jagdishpur, via Madhupur (S.P.) 815353,
Bihar, India.
Editors' note: Aspirin and diarrhoea
Diarrhoea Dialogue 5 (page seven) (page seven) reviewed an article
about aspirin and diarrhoea (The Lancet, 1980, Vol 1: 1329-1330). It advised
against the use of this household remedy because of possible toxic effects, and since it
may distract from the essential treatment - oral rehydration. Dr Steinhoff from India
emphasizes other reasons for not using aspirin in the treatment of diarrhoea. With regard to your review in Diarrhoea Dialogue 5 of the aspirin and diarrhoea
study I wish to point out that the mean difference in daily stool volume between the
aspirin and non-aspirin groups was approximately l00ml. While this may be a statistically
significant difference, I wonder how many paediatricians would consider this a clinically
important difference. This volume of "excess" stool loss could easily be made up
with an extra cup or two of oral rehydration solution. Although no aspirin toxicity was
seen, I doubt if the effect on stool losses is large enough to trouble both the patient
and over-worked ward staff with a six-hourly medication. Mark C Steinhoff, Department of Child Health, Christian Medical College Hospital,
Vellore-632004, India. Rice water Many of the people where I am posted use rice water for babies and children with
diarrhoea. What benefit, if any, does rice water contain? Also, could you suggest some
simple and inexpensive ways that water can be purified in the home? Fuel is very difficult
for our people to obtain. We have the extended family situation so it takes a lot of water
for the needs of each home. Patricia Robertson, B.P. 16, Po, Upper Volta. Editors' note:
On="#page2">page two of this issue we have a report from Singapore on a
study using rice water for rehydrating babies. You can obtain further information from
Professor Wong Hock Boon. For ideas on simple water purification we suggest you contact
Samia Al Azharia Jahn, Water Purification Project, P. O. Box 2681, Khartoum, Sudan (see
her letter on="dd05.htm#page8">page eight of page eight of Diarrhoea Dialogue 5).
|
Midwives in Niger receiving instruction on nutrition during pregnancy.
WHO photograph by R. da Silva
|
 |
(page seven) reviewed an article
about aspirin and diarrhoea (The Lancet, 1980, Vol 1: 1329-1330). It advised
against the use of this household remedy because of possible toxic effects, and since it
may distract from the essential treatment - oral rehydration. Dr Steinhoff from India
emphasizes other reasons for not using aspirin in the treatment of diarrhoea. With regard to your review in Diarrhoea Dialogue 5 of the aspirin and diarrhoea
study I wish to point out that the mean difference in daily stool volume between the
aspirin and non-aspirin groups was approximately l00ml. While this may be a statistically
significant difference, I wonder how many paediatricians would consider this a clinically
important difference. This volume of "excess" stool loss could easily be made up
with an extra cup or two of oral rehydration solution. Although no aspirin toxicity was
seen, I doubt if the effect on stool losses is large enough to trouble both the patient
and over-worked ward staff with a six-hourly medication. Mark C Steinhoff, Department of Child Health, Christian Medical College Hospital,
Vellore-632004, India.
Rice water Many of the people where I am posted use rice water for babies and children with
diarrhoea. What benefit, if any, does rice water contain? Also, could you suggest some
simple and inexpensive ways that water can be purified in the home? Fuel is very difficult
for our people to obtain. We have the extended family situation so it takes a lot of water
for the needs of each home. Patricia Robertson, B.P. 16, Po, Upper Volta.
Editors' note: On="#page2">page two of this issue we have a report from Singapore on a
study using rice water for rehydrating babies. You can obtain further information from
Professor Wong Hock Boon. For ideas on simple water purification we suggest you contact
Samia Al Azharia Jahn, Water Purification Project, P. O. Box 2681, Khartoum, Sudan (see
her letter on="dd05.htm#page8">page eight of Diarrhoea Dialogue 5).
|
In the next issue...
- Diarrhoea Dialogue 7 will focus on the aetiology of
diarrhoea. It will be available at the end of November 1981.
|
Scientific editors Dr Katherine Elliott and Dr William Cutting
Executive editor Denise Ayres Editorial advisory group
Professor David Candy (UK)
Dr I Dogramaci (Turkey)
Professor Richard Feachem (UK)
Dr Michael Gracey (Australia)
Dr Norbert Hirschhorn (USA)
Dr D Mahalanabis (India)
Professor Leonardo Mata (Costa Rica)
Dr Mujibur Rahaman (Bangladesh)
Dr Jon Rohde (USA)
Ms E O Sullesta (Philippines)
Dr Paul Vesin (France)
Dr M K Were (Kenya) With support from WHO and UNDP
|
Issue no. 6 August 1981
Page Navigation
This edition of Dialogue on Diarrhoea Online is produced by Rehydration Project. Dialogue on Diarrhoea was published four times a year in English, Chinese, French, Portuguese, Spanish, Tamil,
English/Urdu and Vietnamese and reached more than a quarter of a million readers worldwide. The English edition of Dialogue on Diarrhoea was produced and distributed by Healthlink Worldwide. Healthlink Worldwide is committed to strengthening primary health care and
community-based rehabilitation in the South by maximising the use and impact
of information, providing training and resources, and actively supporting
the capacity building of partner organisations. - ISSN 0950-0235 Reproducing articles
Healthlink Worldwide encourages the reproduction of
articles in this newsletter for non-profit making and educational uses. Please
clearly credit Healthlink Worldwide as the source and, if possible, send us a copy of any uses made of the material.
|
updated: 23 April, 2014
updated: 23 April, 2014
|






