|
|
Immunisation
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Subject Index | Country Reference | Author Index | Contents of All DD Issues | Issues Menu | Quick Menu | PDF Menu This Issue Navigation |
version of this Issue
|
There is much information in this issue that is valuable
and useful. Online readers are reminded, however, that treatment guidelines and health
care practices change over time. If you are in doubt, please refer to
WHO's up-to-date Dehydration Treatment
Plans. |
Pages 1-6 Immunisation
A supplement to Dialogue on Diarrhoea Online Issue 30 - September 1987
|
DDOnline Immunisation
supplement to DD30
1. R. G. Feachem and M. A. Koblinsky: Interventions for the control of diarrhoeal diseases among young children: measles immunisation. Bulletin WHO 61,641-652, 1983. |
|
DDOnline Immunisation
supplement to DD30
|
WHO's EPI has estimated that coverage rates for the vaccines in children under one
year old in developing countries (excluding China) are as follows:
|
Who should be immunised and at what age? Infants and children All children should be immunised against the preventable childhood diseases. The="#schedule">immunisation schedule describes the number of times that a child needs to be given vaccinations and how far apart each visit should be. Following the ideal schedule, each child should be fully immunised by the age of nine months, or soon after, because infants are at greater risk from these diseases. Many countries try to immunise all children under five years of age who may be at risk. Women Neonatal tetanus is prevented for several years by immunising women of child-bearing age with at least two doses of tetanus toxoid. After five doses of tetanus toxoid all children born subsequently are protected from neonatal tetanus. A woman who received three doses of DPT as a child will greatly increase her infants' protection by two boosters (ideally before or during early pregnancy) when she is ready to bear children. (Hygienic cord treatment can also prevent neonatal tetanus but is not as effective as complete immunisation of the mother.) |
A schedule recommended by WHO
to assure protection at an early age is as follows:
|
Simplified schedule for remote populations (two contacts as used in parts of West Africa |
||
| Age | Vaccine | Reason |
| All children 3-8 months old | DPT(1)-IPV(1), BCG | IPV in two doses is protective against paralytic polio. |
| All children 9-14 months old | DPT(2)-IPV(2), measles | In remote areas the average age of contracting measles is delayed to the second and third years of life and later vaccination is still effective. |
| N.B. IPV: Inactived Poliovirus Vaccine DPT-IPV may be obtained in a single preparation EPI also recommends that OPV be added to this schedule. |
||
Semi-annual single day 'pulse' campaigns (as used in Brazil) |
||
| Age | Vaccine | Reason |
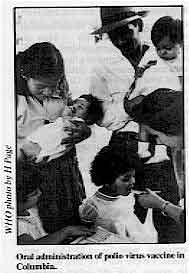
| All children 0-59 months old | OPV (up to 10 doses) | After regular vaccination with OPV vaccine, the vaccine virus replaces the naturally occurring disease-causing virus in the environment. |
| All children 9-23 months old | measles (up to 2 doses) | Giving a second dose of measles vaccine increases effective coverage. |
| All children 2-11 months old | DPT (2 doses) | Third DPT through regular primary health care services in clinics; 2 doses of DPT are partially effective (50-60%) against pertussis. |
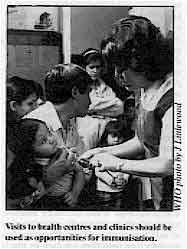
Can a sick child he immunised? Mothers sometimes do not bring a sick child for immunisation and if they do, health workers frequently do not immunise them. Mothers and health workers need to know that all EPI immunisations are safe and effective even if a child is ill with fever, diarrhoea, vomiting, or respiratory infection. No chance should be missed to immunise a child. This is a recommendation of the EPI. The benefits of immunisation far outweigh the risks, especially in malnourished children. Only in very few exceptional cases is it not advisable to immunise. For example, a child who has had a severe reaction to DPT (fits, extreme crying) should not be given pertussis immunisation, but should get diphtheria-tetanus vaccine. |
|
DDOnline Immunisation
supplement to DD30
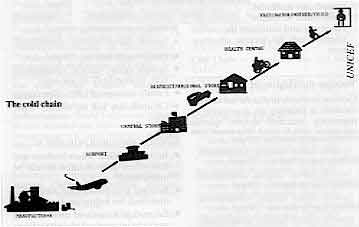
Vaccine storage Each vaccine needs to be kept at the correct temperature to keep it safe, effective and
stable. Live polio and measles vaccines are most sensitive to heat, tetanus toxoid least
sensitive. |
Recommended storage temperatures and times are shown below: |
||||
| Level: | Central store | Regional Health Centre | Transport | |
| Maximum time: | Upto 8 months | Upto 3 months | Upto 1 month | Upto 1 week |
| Measles Oral polio virus |
-15° C to -25° C |
less than +8° C |
||
| DPT Tetanus toxoid BCG |
+2° C to +8° C +2° C to +8° C less than +8° C |
|||
| NB: DPT and tetanus toxoid must never be frozen. | ||||
Lack of, or irregular electricity supply, poor quality kerosene, and unreliable vehicles may cause the cold chain to break down.
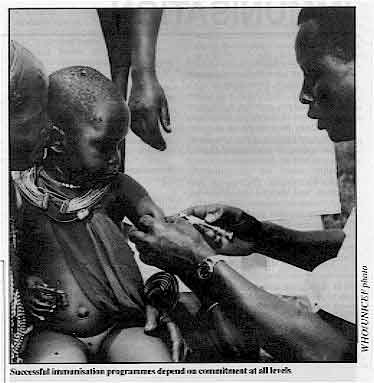
Community problems Communities must be involved in the decision to implement immunisation programmes. Families must want to have their children immunised and know, why immunisation is important. It is equally important that they know that children may suffer mild side effects from the vaccinations. Specific problems may include:
In a survey carried out in a Latin American country of 1,145 children, children had not been taken for immunisation or had not completed a series of immunisations because:
Health workers need to be able to:
|
|
DDOnline Immunisation
supplement to DD30
|
|
DDOnline Immunisation
supplement to DD30
RESOURCE LIST SOURCES OF INFORMATION AND EQUIPMENT
BOOKS/MANUALS AHRTAG, Battersby A. How to chose and make a cold box, 1984. AHRTAG, Elford J. How to look after a refrigerator, 1980, 1983 (revised edition). Child Alive, Learn more about immunisation, League of Red Cross and Red Crescent Societies, 1986. Dick B, Issues in immunisation in developing countries: an overview, EPC 1985. Expanded Programme on Immunization, The Cold Chain Product Information Sheets, WHO/UNICEF. 1987. Favin. M., Sabin. E., and Stinson. W. Immunizations, World Federation of Public Health Associations, Geneva, May 1984. Heggenhougen K, and Clement J, Acceptability of childhood immunization: social science perspectives, EPC, 1987. Johns Hopkins University, Population Information Program, Immunizing the World's Children, Population Reports, Series L, Number 5, March-April 1986, Issues in World Health. King M. et al, Primary Child Care, Vols I and II, TALC, 1978. Liberia, Ministry of Health and Social Welfare, EPI Handbook for Healthworkers, 1982, EPI, P. O. Box 3600, Monrovia, Liberia. POLIOPLUS PROGRAM, The Challenge, An Action Guide for National POLIOPLUS Projects, 1987,Rotary International. Rockefeller Foundation, Protecting the World's Children: Vaccines and Immunization, (Presented at the Bellagio Conference, March 13-15, 1984,) New York, 1984. The Task Force for Child Survival, Protecting the World's Children: Bellagio II, (Presented at the Cartagena Conference, October 14-16, 1985) Decatur, GA, 1986. UNICEF, The State of the World's Children, 1986, Oxford University Press, 1986. UNICEF, Universal Child Immunization by 1990, Assignment Children 69/72, 1985. WHO, Immunization in Practice: A Guide for Health Workers Who Give Vaccines, WHO Training Course. WHO, Logistics and Cold Chain for Primary Health Care, WHO Training Course. WHO, Technician's Handbook for Compression Refrigerators, WHO Training Course. WHO, Training Course for Mid-Level Managers, WHO Training Course. WHO, Training Course on Planning and Management, WHO Training Course.
ARTICLES Haaga, J. Cost-effectiveness and Cost-benefit Analysis of Immunization Programmes in Developing Countries in Jelliffe, D. and Jelliffe, E. eds., Advances in International Maternal and Child Health, v. 6, Oxford University Press, New York, 1986. Feachem R. G. and Koblinsky. M. A. Interventions for the Control of Diarrhoea1 Diseases Among Young Children: Measles Immunization, Bulletin of the World Health Organization 61(4), 1983, p. 641-652. Foster, S. O., Immunizable and Respiratory Diseases and Child Mortality Population and Development Review, Fall Supplement 1984.
AUDIOVISUALS Cold Chain -Target Diseases, (24 slides) TALC. Cold Chain, (24 slides) TALC. Primary Child Care, (240 slides) TALC. Severe Measles, (24 slides) TALC.
NEWSLETTERS ARI News, AHRTAG. Child Alive Newsletter, League of Red Cross and Red Crescent Societies. EPI Cold Chain Update, WHO. EPI Newsletter, Expanded Programme on Immunisation, PAHO, 525 23rd Street, NW, Washington, DC 20037, U. S. A. Feedback, International Health Program Office, Centers for Disease Control, Public Health Service, Department of Health and Human Services, Atlanta, GA, 30333, U. S. A. Future, UNICEF Regional Office for South East Asia, UNICEF House, 73 Lodi Estate, New Delhi 110003, India. Immunisations, International Children's Centre, Paris. WeekIy Epidemiological Bulletin, WHO. World Immunization News (WIN), The Task Force for Child Survival, 1989 North Williamsburg Drive, Suite I, Decatur, GA 30033, U. S. A. Acknowledgement This information has been prepared by REACH (Resources for Child Health), Ninth Floor, 1100 Wilson Boulevard, Arlington, VA 22209, U.S.A. DD would particularly like to thank Pierre Claquin, Norbert Hirschhorn, Cynthia Rawn, Paul Steele, and Robert Steinglass. REACH is a project of John Snow incorporated, a contractor to the United States Agency for International Development (AID), providing short- and long-term technical assistance in immunization and health care financing, and primary health care systems support to countries assisted by AID.
Produced by Dialogue on Diarrhoea with support from the REACH project
|
Immunisation
Health Update - A supplement to Issue no. 30 September 1987
|
This edition of Dialogue on Diarrhoea Online is produced by Rehydration Project. Dialogue on Diarrhoea was published four times a year in English, Chinese, French, Portuguese, Spanish, Tamil, English/Urdu and Vietnamese and reached more than a quarter of a million readers worldwide. The English edition of Dialogue on Diarrhoea was produced and distributed by Healthlink Worldwide. Healthlink Worldwide is committed to strengthening primary health care and community-based rehabilitation in the South by maximising the use and impact of information, providing training and resources, and actively supporting the capacity building of partner organisations. - ISSN 0950-0235 Reproducing articles Healthlink Worldwide encourages the reproduction of articles in this newsletter for non-profit making and educational uses. Please clearly credit Healthlink Worldwide as the source and, if possible, send us a copy of any uses made of the material. |
updated: 23 August, 2019
updated: 23 August, 2019